Endocrine Emergencies.
A 73yr old lady presents with confusion and agitation. She is found to have a BSL of 1.2mmol/l. Which of the following is the most appropriate treatment?
50mls of 50% Dextrose is 25gms of sugar. (A standard Mars bar has 21.8 gms of sugar). And no---"Rectosweet" does not exist.
A 48yr old woman with a history of Grave's disease presents with confusion, fever and a sinus tachycardia of 140/min. You clinically think she has a thyroid storm. Which of the following is not part of her early treatment in the ED?

NSAIDs including Aspirin displaces thyroxine from circulating proteins so can make the situation worse. Watch for hypoglycemia so add Glucose to IV fluids. Propylthiouracil blocks conversion of T4 to T3. After blockage by Propylthiouracil give iodine as Potassium Iodide, Sodium Iodide or Lugols Iodide. Oh yes also give Hydrocortisone 100mg IV.
A previously well 16yr old girl presents from the LMO with a BSL of 40mmol/l. Which of the following would you NOT expect?

In DKA the osmotic diuretic effect of the elevated circulating glucose will cause her to become dehydrated and deplete electrolytes like K and PO4. Keto and lactic acids will cause a metabolic acidosis and her compensatory response to this will be to increase her respiratory rate. Her breath will likely smell like acetone.
Following recent back surgery a 36yr old lady presents with nausea, mild confusion and hypotension. She has been on long term steroids for SLE. You suspect an acute adrenal crisis. How would you treat it?

The adrenal gland releases Aldosterone and Cortisol from its cortex (which is why they are called "Adrenocortical hormones". In patients on long term oral steroids an adrenal crisis may be precipitated by a recent stress---like having surgery. The hypotension requires IV fluid and hydrocortisone. Watch for low glucose. Electrolytes may show a low Sodium and high Potassium.
The famous wrestler "Andre the Giant" had Gigantism. Which of the following statements about him is INCORRECT?
He was a heavy drinker---apparently once he drank 116 beers in 6 hours. He passed out and couldnt be moved so was left in the lobby of the hotel with a piano cover over him to sleep it off.
What does the endocrine tumour "Pheochromocytoma" secrete?
Classically people present with the triad of episodic headache, sweating and tachycardia. The primary treatment is surgical, which can be finicky to say the least.
Which of the following would you NOT expect in a Myxoedema (hypothyroid) crisis?

Will usually be precipitated, most commonly, by infection in a patient with an underlying thyroid problems (like a patient with a thyroidectomy on replacement Thyroxine). Supportive treatment---A,B,C. Hydrocortisone 100mg IV then T4 (Levothyroxine) 200 to 400mic IV is a good start. Watch for Hypoglycemia and Hyponatremia. Consult early to an endocrinologist and likely with ICU.
A 64yr old man presents with hypertension, muscle aches and general weakness. The image shows his VBG taken. His serum Na was elevated at 152 mmol/l. What Endocrine condition does he most likely have?
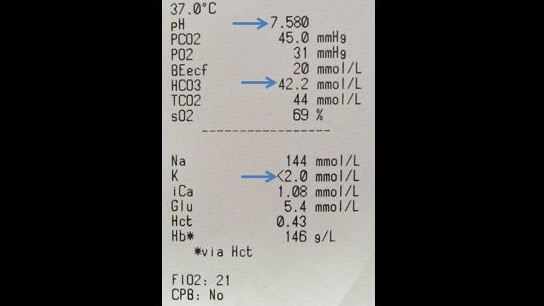
Aldostrone resorbs Na in the distal convoluted tubules and pees out K+ and H+. As a result you get high serum Na and low K+ as well as an alkalosis because of the loss of H+. You get hypertension. Most of the time it is caused by a small adrenal tumour that can be surgically removed.
A 73yr old lady presents with peri oral paresthesia, restlessness and mild confusion a few days after a thyroidectomy. What did the blood test confirm?
She has hypocalcemia because some (or all) or her parathyroid glands were accidentally removed at surgery. This means her parathyroid hormone will not be able to do its job, which is resorb calcium from the intestines and kidneys as well as releasing calcium from bones. She will also be hyper reflexic and may have carpopedal spasms or even trismus. Initial treatment in ED---Calcium IV---as 10% Ca gluconate or 10% Ca Chloride.
What endocrine disorder did President John F Kennedy suffer from?
His swarthy tan was as much to do with his Addison's disease as the sun. He was diagnosed with Addison's in the 1940s then hypothyroidism in 1955. The running theory now is that these were caused by him having a rare autoimmune disease called APS2.